
Hydroponic Grow Systems
World's Easiest & Most Effective Hydroponic Grow Systems, Hydroponic Setups, & Hydroponic Designs. SuperPonic Systems Give You A Fusion of Proven Hydroponic Methods, Maximizing Yields & Minimizing Maintenance.
















Need help?
Frequently Asked Questions
Hydroponic Systems: A Gateway to a Healthier and More Sustainable Lifestyle
Innovations in agriculture have continually pushed the boundaries of traditional farming methods. One such groundbreaking technique that has gained immense popularity in recent years is hydroponics. This method revolutionizes the way we grow plants by eliminating soil and utilizing nutrient-rich water solutions to foster plant growth.
Let’s delve into what hydroponic systems entail and how they are reshaping modern agriculture.
What is a Hydroponic System?
In essence, hydroponics is a soilless cultivation method that relies on water-based nutrient solutions to grow plants. Instead of soil, plants are rooted in various inert mediums such as perlite, coconut coir, or rockwool. The essential nutrients required for plant growth are dissolved in water, creating a balanced solution that is delivered directly to the plant roots.
Types of Hydroponic Systems
There are several types of hydroponic systems, each with its unique characteristics and advantages:
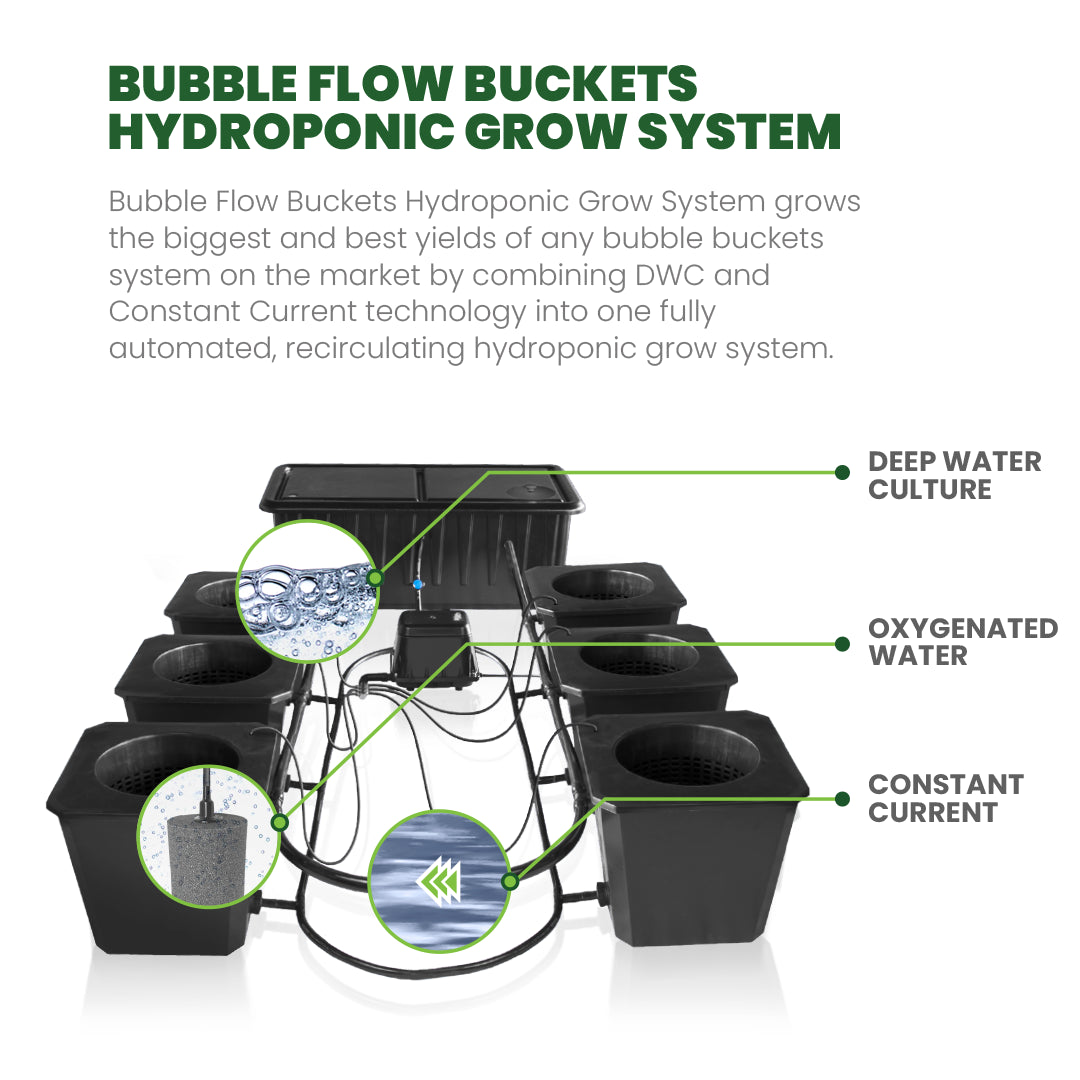
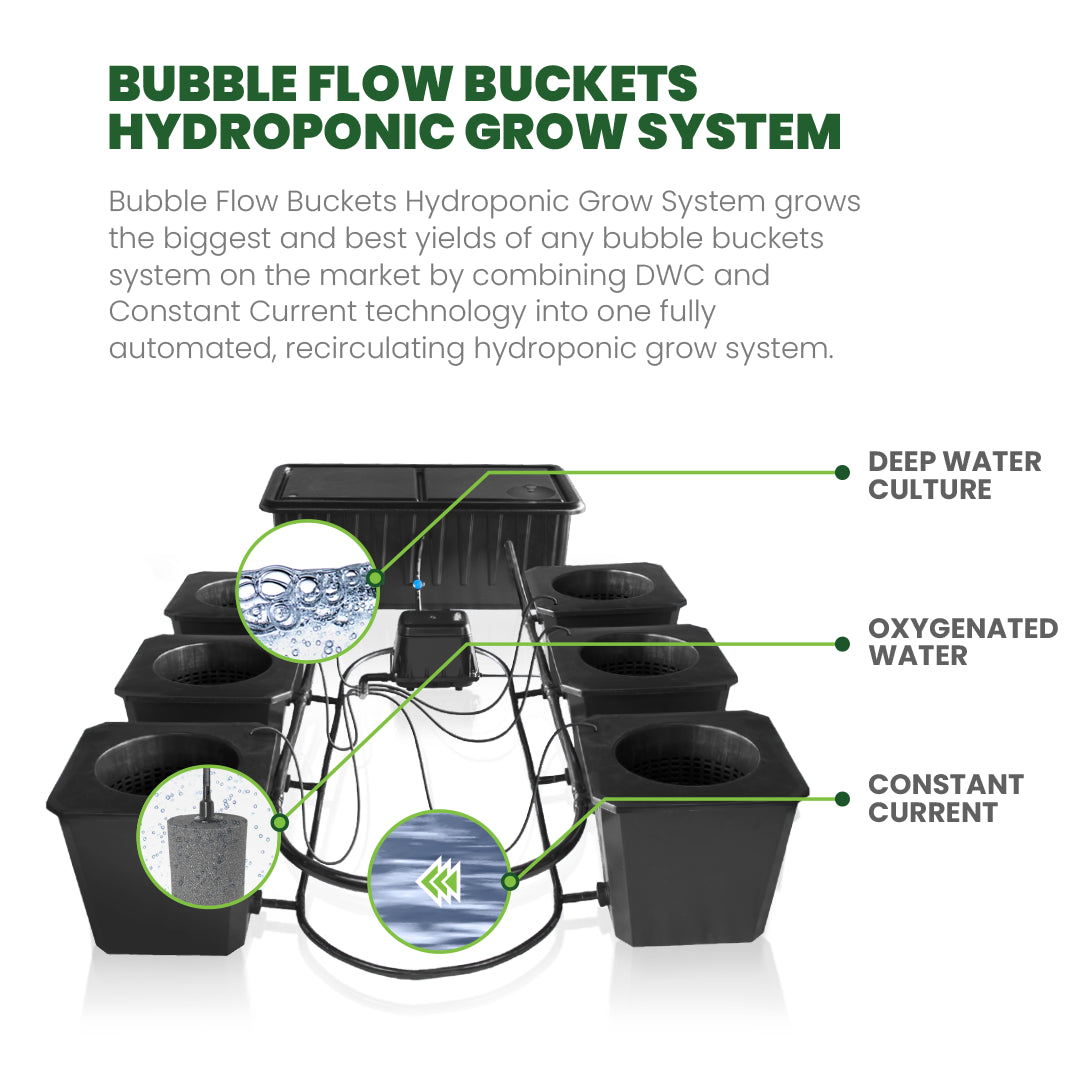
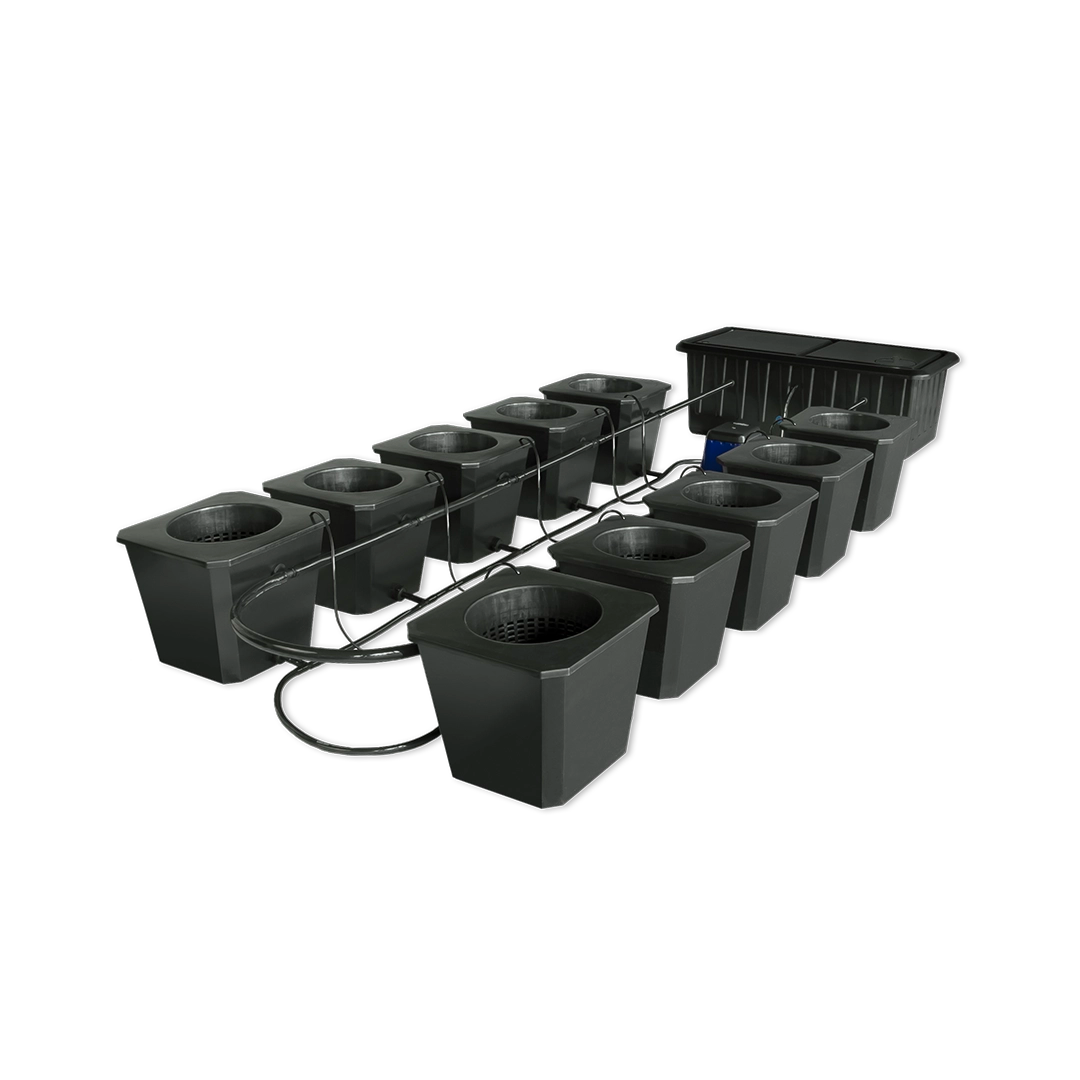
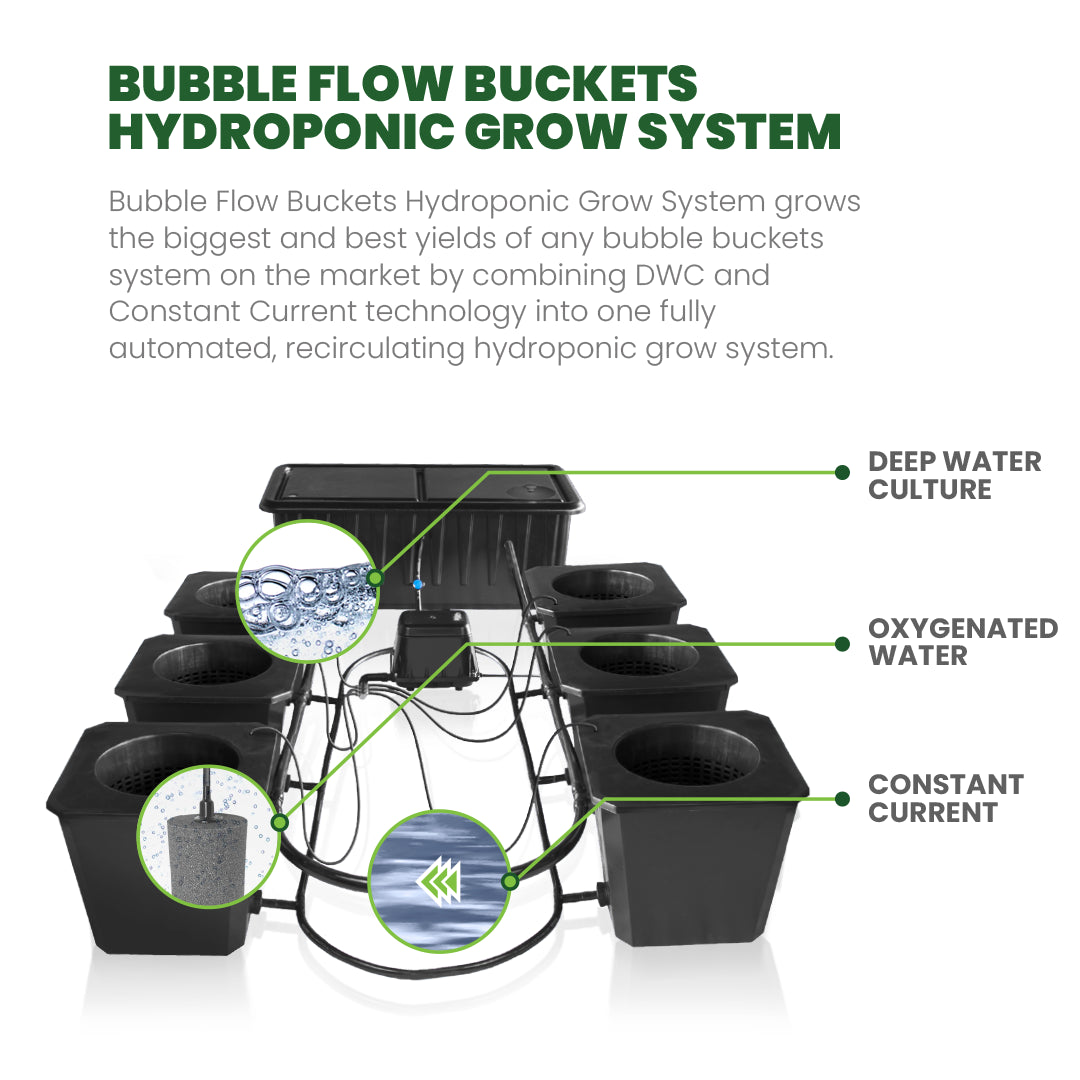
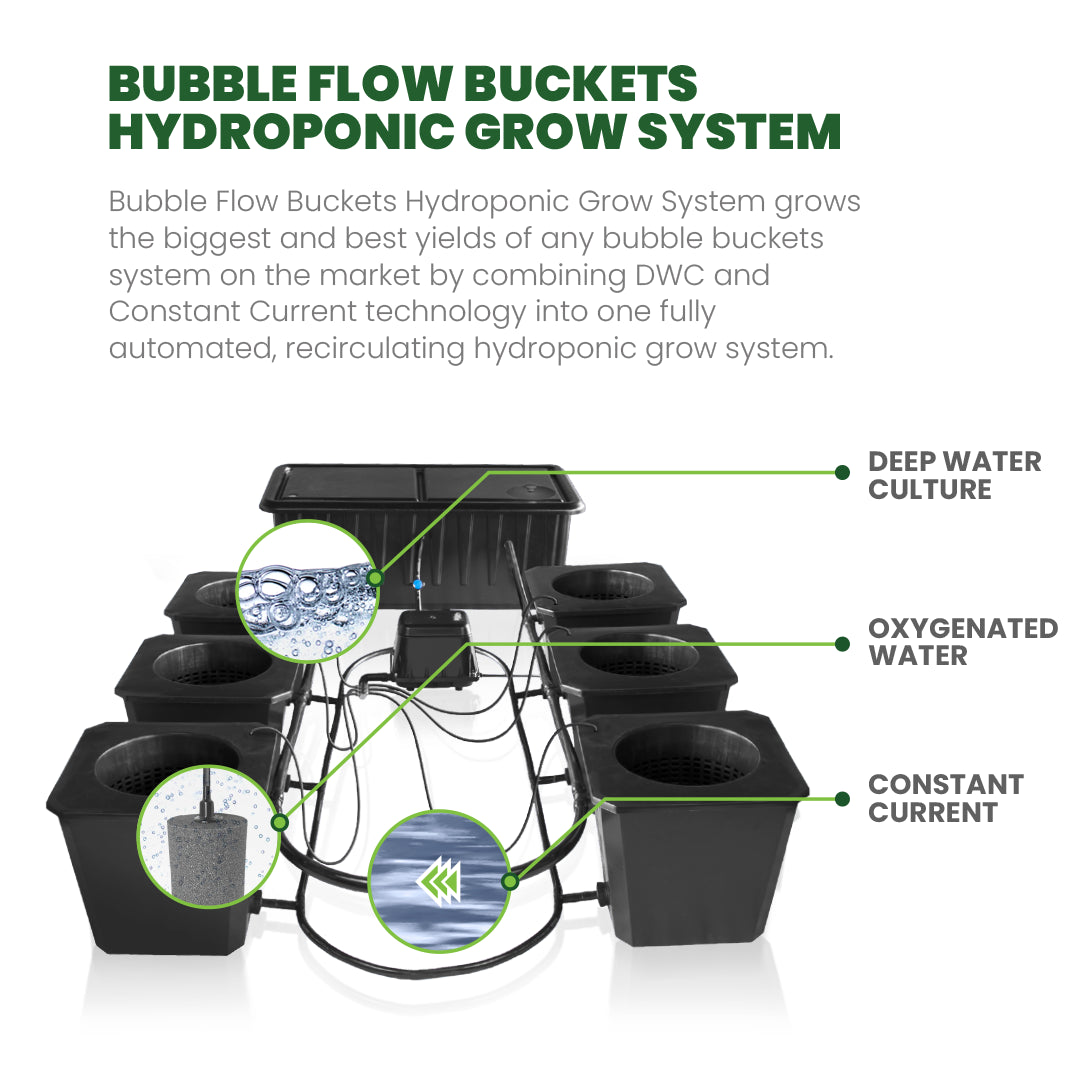
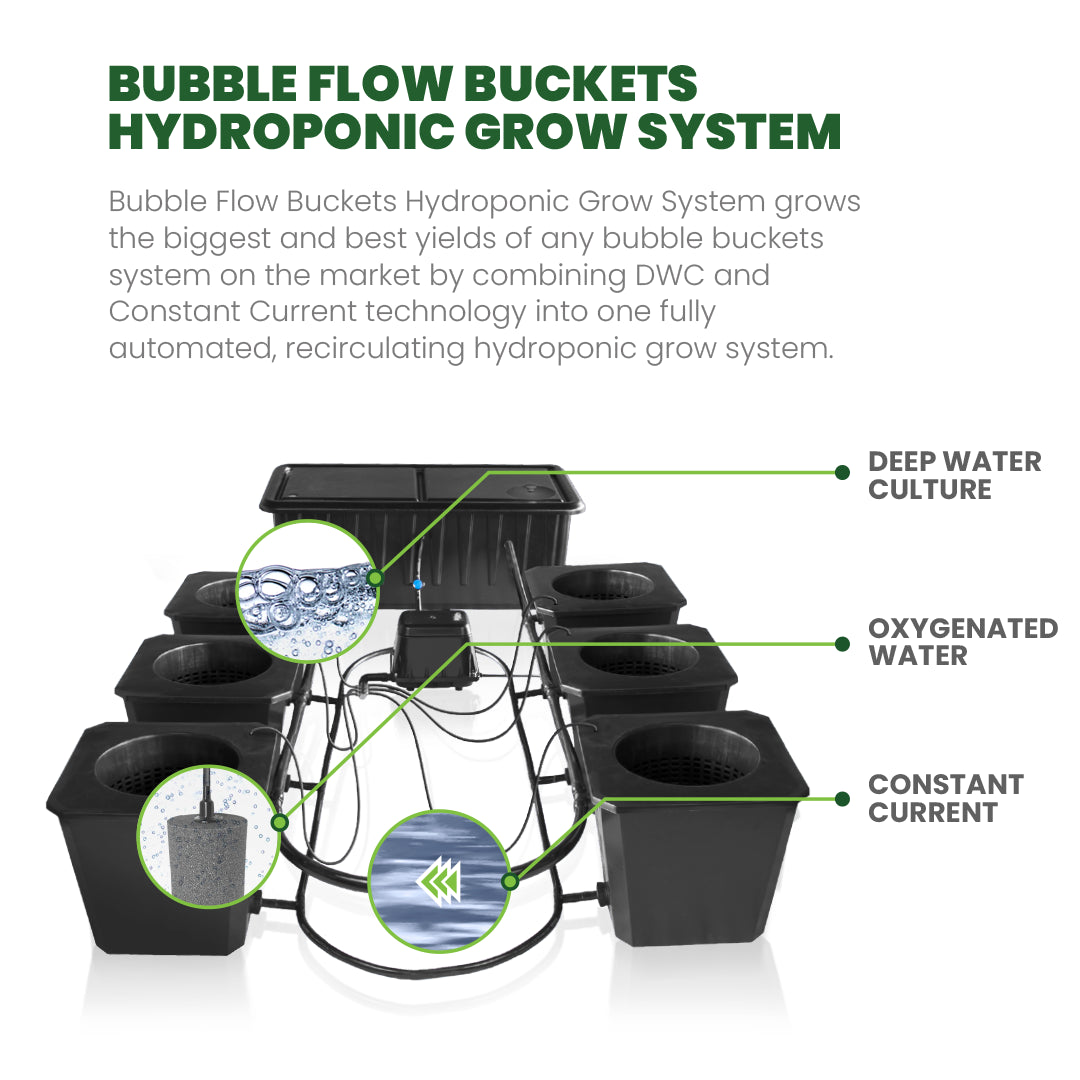
Deep Water Culture (DWC): This method involves suspending plant roots in a nutrient solution with an oxygenating system to ensure adequate oxygen levels.
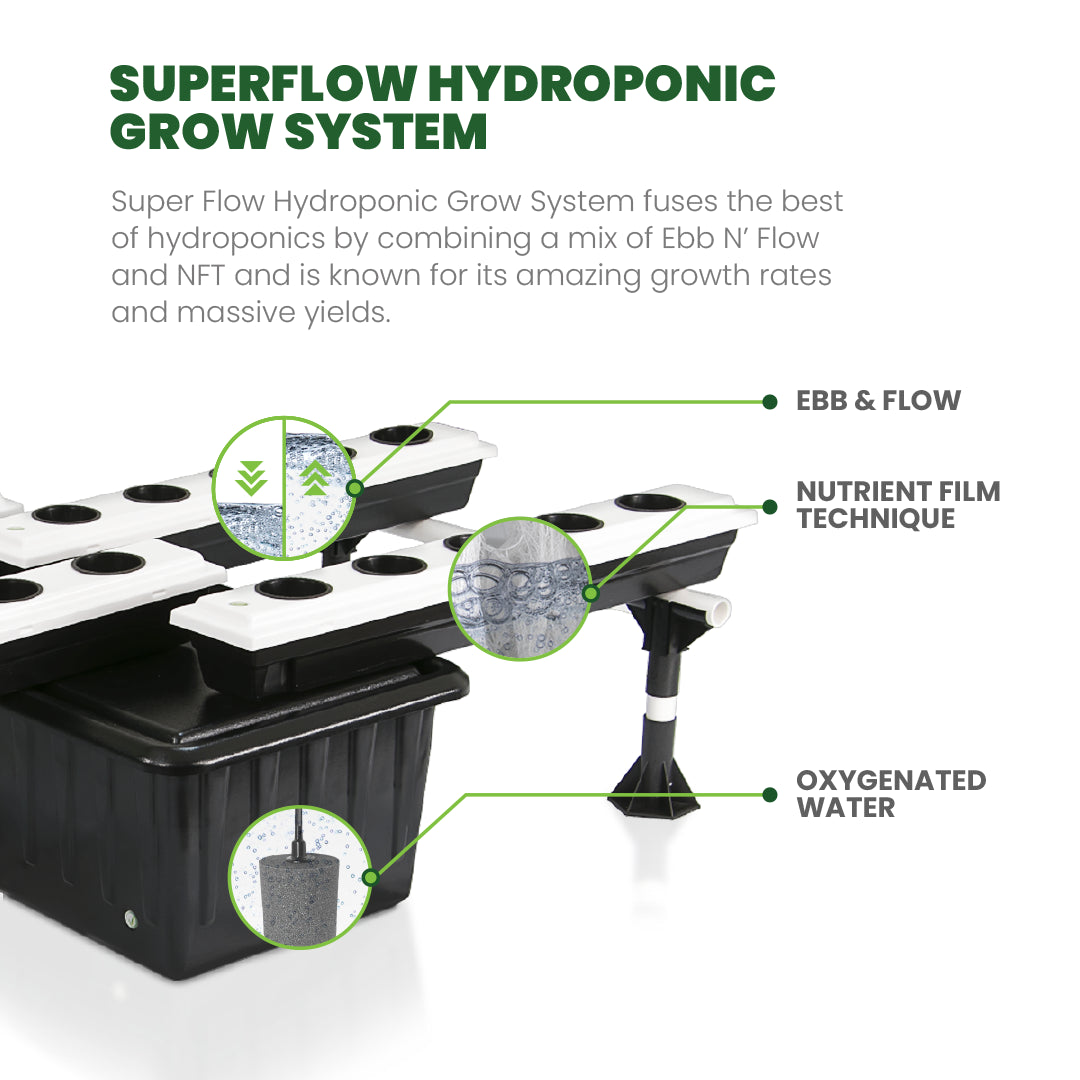
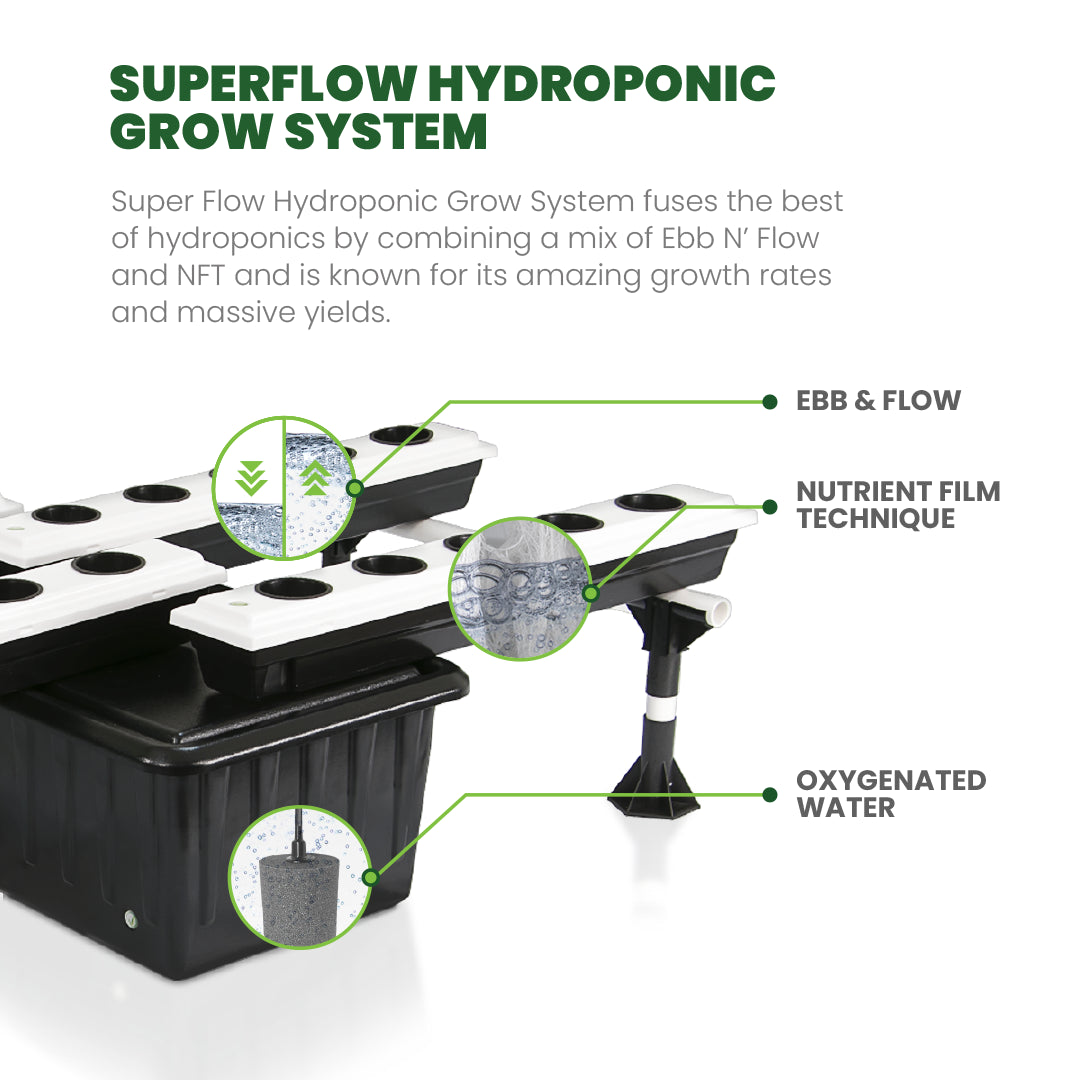
Nutrient Film Technique (NFT): Here, a thin film of nutrient-rich water flows over the plant roots, allowing them to absorb nutrients while being exposed to air.
Ebb and Flow (or Flood and Drain): In this system, the nutrient solution periodically floods the plant roots and then drains away, providing both nutrients and oxygen.
Drip System: Nutrient solutions are dripped onto the plant roots through a network of tubes or pipes, providing a controlled and consistent supply of nutrients.
Aeroponics: This method involves suspending plant roots in the air and misting them with a nutrient solution, ensuring maximum exposure to oxygen and nutrients.
Benefits of Hydroponic Systems
Water Efficiency: Hydroponic systems use significantly less water compared to traditional soil-based farming, as water is recirculated within the system.
Faster Growth Rates: With direct access to nutrients and optimized growing conditions, plants in hydroponic systems tend to grow faster than those in soil.
Space Saving: Hydroponics allows for vertical farming and can be set up indoors, making it ideal for urban areas or locations with limited space.
Controlled Environment: Nutrient levels, pH, and other environmental factors can be precisely controlled, leading to healthier plants and higher yields.
Year-Round Growing: Unlike traditional farming, hydroponics isn’t bound by seasonal limitations, enabling year-round cultivation regardless of external weather conditions.
Crop Variety: Hydroponics allows for the growth of a wide variety of plants, from leafy greens and herbs to fruits and vegetables, providing diverse options for cultivation.
Advanced Techniques in Hydroponics
Vertical Farming: Hydroponic systems are exceptionally suitable for vertical farming, maximizing space utilization by stacking layers of plants. This method significantly increases crop yield per square meter of land.
Aquaponics: Integrating aquaculture with hydroponics, aquaponic systems utilize fish waste to provide nutrients for plants, creating a symbiotic relationship between fish and crops.
Closed-Loop Systems: These systems aim to minimize resource waste by recycling water and nutrients, creating a more sustainable and efficient growing environment.
Challenges of Hydroponics Systems
While hydroponics offers numerous advantages, there are challenges to consider, such as initial setup costs, the need for technical expertise, and the risk of system failures impacting plant health.
While hydroponics can reduce pest issues, diseases and pests can still affect crops. Innovative solutions like integrated pest management and biological controls are being explored to mitigate these risks.
The energy required to power indoor hydroponic systems can be a concern. Advances in energy-efficient lighting (such as LED technology) and renewable energy sources aim to address this issue.
Hydroponic Systems: Cultivating a Greener Future
Reduced Environmental Impact: Hydroponic systems require fewer pesticides and herbicides compared to traditional farming, minimizing chemical runoff that can harm ecosystems.
Conservation of Arable Land: With the ability to grow vertically and indoors, hydroponics reduces the need for expansive farmlands, preserving natural habitats.
Integration with Renewable Energy: The integration of hydroponics with renewable energy sources like solar power could further enhance its sustainability and reduce operating costs.
Hydroponic systems represent a promising avenue for sustainable and efficient agriculture. By minimizing resource use and maximizing yield, these innovative systems are reshaping the future of farming.
As technology continues to advance, the integration of hydroponics into mainstream agriculture holds immense potential to address food security challenges while minimizing environmental impact.
Explore the world of hydroponics, and witness firsthand how this innovative method is transforming the way we grow food.
What is the Most Effective Hydroponic System?
What is a Hydroponic System?
A hydroponic system is a method of growing plants without soil, where plants receive their nutrients directly from water mixed with a mineral nutrient solution. This approach allows for precise control over the plant's environment, optimizing conditions for growth. Instead of relying on soil to deliver nutrients, hydroponics uses various mediums like perlite, coconut coir, rockwool, or simply water to support the plant's root system.
In hydroponic systems, the nutrient solution is typically circulated or periodically applied to the plant roots. There are different types of hydroponic systems, each with its own way of delivering nutrients and water.
Choosing the most effective hydroponic system depends on various factors like space availability, budget, level of expertise, and the specific needs of the plants you're growing.
Unraveling the Most Effective Hydroponic Systems for Your Lush Garden
Here's a breakdown of some popular hydroponic systems and their strengths:
Deep Water Culture (DWC): DWC is straightforward and great for beginners. Plants are suspended in a nutrient solution with an air pump providing oxygen to the roots. It's cost-effective and low-maintenance but requires monitoring water levels and pH.
Nutrient Film Technique (NFT): This system involves a continuous flow of nutrient solution down a sloped tray where plant roots are exposed. NFT is efficient in water usage and suitable for smaller plants with shallow roots. However, it needs a consistent flow of nutrients, and power outages can be problematic.
Ebb and Flow (Flood and Drain): This system floods the plant roots with a nutrient solution intermittently and then drains it back to a reservoir. It's versatile, accommodating various plants, and doesn't require constant nutrient flow. However, it needs a timer and can be prone to system failures if not properly maintained.
Aeroponics: Aeroponic systems mist plant roots with a nutrient solution. They use minimal water and are efficient for faster growth due to increased oxygenation at the root level. Yet, they require precise misting intervals and are more complex to set up.
Drip System: This system provides a slow and steady drip of nutrient solution to plant roots through tubing or emitters. It's versatile, adaptable to various plant sizes, and is relatively easy to set up. However, it can be prone to clogging and may need regular maintenance.
Vertical Hydroponics: This system maximizes space by growing plants vertically. It's efficient for those with limited space, allowing for higher plant density. However, it requires adequate lighting and careful attention to watering and nutrient distribution.
Wick System: Wick systems are simple and passive, using a wick to deliver nutrients to plant roots from a reservoir. They're low-cost and easy to set up but might not be suitable for larger plants or those needing more nutrients.
Aquaponics: Aquaponics combines hydroponics with aquaculture (raising fish). Fish waste provides nutrients for plants, and plants filter the water for the fish. It's a sustainable, symbiotic system but requires expertise in both hydroponics and aquaculture.
Dutch Bucket System: Ideal for larger plants like tomatoes, cucumbers, or peppers, this system uses individual buckets filled with a growing medium where plants are grown. The nutrient solution is delivered via tubes, allowing for more control over individual plants' nutrient needs.
Fogponics: Similar to aeroponics, fogponics uses ultrasonic foggers to create a fine mist of nutrient solution. It enhances oxygenation but may require more specialized equipment.
Kratky Method: This passive system doesn't use pumps or electricity. Plants are placed in a container with a nutrient solution, and as the solution is used, the roots grow deeper to access it. It's simple but best suited for smaller plants with shorter growth cycles.
Choosing the most effective system involves considering factors like space, budget, plant type, and your level of involvement. Some systems might be better suited for commercial setups, while others are perfect for hobbyists or home growers.
Experimentation and understanding your plants' needs are key to finding the most suitable hydroponic system for your goals.
A hydroponic system is a method of growing plants without soil, using a nutrient-rich water solution to deliver essential minerals and nutrients directly to the plant roots. Instead of relying on soil to provide nutrients, hydroponics uses various mediums such as perlite, clay pellets, rockwool, or even just water to support the plant roots while the nutrient solution is delivered.
There are several types of hydroponic systems, each with its own way of delivering water and nutrients to the plants:
Hydroponics Made Easy: Choosing the Perfect System for Beginners
Hydroponics can be an exciting and efficient way to grow plants! When starting out, selecting the right system for beginners is crucial.
Here are a few simple hydroponic systems suitable for newcomers:
Deep Water Culture (DWC): This is one of the easiest systems for beginners. Plants are suspended in a solution of nutrient-rich water. An air pump and airstone oxygenate the water, providing nutrients to the roots.
Nutrient Film Technique (NFT): This system involves a continuous flow of nutrient solution over the plant roots. It's a simple setup, though it requires a bit more monitoring to ensure the flow remains consistent.
Wick System: This is the most straightforward and least expensive. It operates by using a wick to passively transport nutrient solution from a reservoir to the plants' roots. It's low-maintenance but might not be as suitable for larger plants.
Ebb and Flow (Flood and Drain): Plants sit in a growing medium and are periodically flooded with nutrient solution from a reservoir. It's relatively simple to set up and manage.
What to Consider When Choosing Your Hydroponic System?
Selecting a hydroponic system involves various considerations that can significantly impact your success. Here are key factors to keep in mind:
Space availability: Different systems have varied space requirements. Consider the area you have and choose a system that fits comfortably within that space.
Budget: Costs can vary widely between systems. Some are more cost-effective but might require more maintenance, while others could be pricier but more automated.
Skill level: Certain systems might be more user-friendly for beginners, while others might require more expertise in terms of setup and maintenance.
Type of plants: Certain systems are better suited for specific types of plants. For instance, some are ideal for leafy greens, while others may be better for fruiting plants like tomatoes or peppers.
Maintenance requirements: Consider the time and effort you're willing to put into maintenance. Some systems require more attention than others, especially when it comes to monitoring pH levels, nutrient solutions, and cleaning.
Water and nutrient circulation: Different systems have distinct methods of delivering water and nutrients to the plants. Some use continuous flow, while others might use intermittent cycles. Choose one that aligns with your preferences and resources.
Control over environmental factors: Some systems offer better control over variables like temperature, humidity, and light. If environmental control is crucial for your plants, select a system that allows for this level of manipulation.
Scalability: Consider whether you want a system that can be easily expanded in the future if you plan to grow more plants.
Energy efficiency: Certain systems might consume more power than others. Consider the energy requirements and choose a system that aligns with your energy-saving goals.
Aesthetics and design: Some systems are more visually appealing or can be integrated into your home decor more seamlessly. If aesthetics matter to you, factor this into your decision-making process.
By considering these aspects, you can narrow down the options and select a hydroponic system that best aligns with your needs, resources, and growing goals.
How Do I Choose a Hydroponic System?
Hydroponics is a soilless method of growing plants in a nutrient-rich water solution. There are many different types of hydroponic systems, each with its own advantages and disadvantages.
Choosing a hydroponic system depends on various factors, including your space, budget, what you want to grow, and your comfort level with managing the system.
Factors to Consider When Choosing a Hydroponic System
Here are some key points to consider:
System Type: There are several types of hydroponic systems like Deep Water Culture (DWC), Nutrient Film Technique (NFT), Ebb and Flow (or Flood and Drain), Drip Systems, Aeroponics, and more. Each has its own pros and cons. Research each type to understand their workings and decide which aligns best with your needs.
Crop Selection: Certain systems are better suited for specific types of plants. For instance, NFT systems work well for smaller plants with shallow roots, while DWC systems are good for larger plants that need more support.
Complexity and Maintenance: Evaluate how much time and effort you're willing to put into maintenance. Some systems require more attention to maintain nutrient levels, pH balance, and water circulation, while others are more automated.
Water and Nutrient Management: Different systems have varying requirements for water and nutrient management. Some may need more frequent monitoring and adjustments to maintain optimal levels of nutrients and pH, while others might have more automated or self-regulating features.
Growth Rate and Yield: Consider the expected growth rate and yield of the plants you want to grow. Some systems may support faster growth rates or higher yields compared to others.
Energy Efficiency: Certain systems might be more energy-efficient than others. For instance, aeroponic systems often use less water and energy compared to traditional soil-based methods or some other hydroponic systems.
Noise and Space Requirements: Some systems, especially those involving pumps or aeration, might produce more noise. Consider this factor if the system will be located in a place where noise could be an issue.
Consider the space where you plan to set up the system. Some systems are compact and suitable for small areas (like countertop units), while others might require more space. Additionally, some systems might require more vertical space, so consider the height clearance needed.
Budget: Different systems come with varying costs. Assess your budget and find a system that fits within it. Remember to consider ongoing expenses like nutrient solutions, electricity, and replacement parts.
Experience Level: If you're new to hydroponics, starting with a simpler system might be beneficial. However, if you have experience or are comfortable with technology and plant management, you might opt for a more advanced system.
Climate and Environment: Consider your local climate and environment. Some systems might need additional climate control or might not be suitable for extreme temperatures or humidity levels.
Availability of Supplies: Check the availability of supplies and replacement parts for the system you choose. It's beneficial to have easy access to things like growing mediums, pumps, and specific components.
Aesthetics and Design: Depending on where you plan to set up your hydroponic system, aesthetics might be important. Some systems are designed to be visually appealing and could be suitable for display indoors.
Research and Reviews: Look for reviews and experiences of others who have used the systems you're interested in. This can give you insights into real-world performance and potential issues.
Future Expansion: Think about whether you might want to expand your system in the future. Some systems are easier to scale up than others.
Support and Resources: Check if there are resources, guides, or communities available that can help you with the chosen system. Having support when troubleshooting issues can be invaluable.
Ultimately, there isn't a one-size-fits-all answer. It's about finding a balance between what suits your needs, resources, and comfort level. If possible, consider starting with a smaller setup or experimenting with different systems before committing to a larger, more permanent one.
No matter which system you choose, be sure to do your research and make sure that you understand how to use it properly. Hydroponics can be a rewarding and fun way to grow your own food, but it is important to start with a system that is right for you.